How to choose the right coronary stent?
Introduction
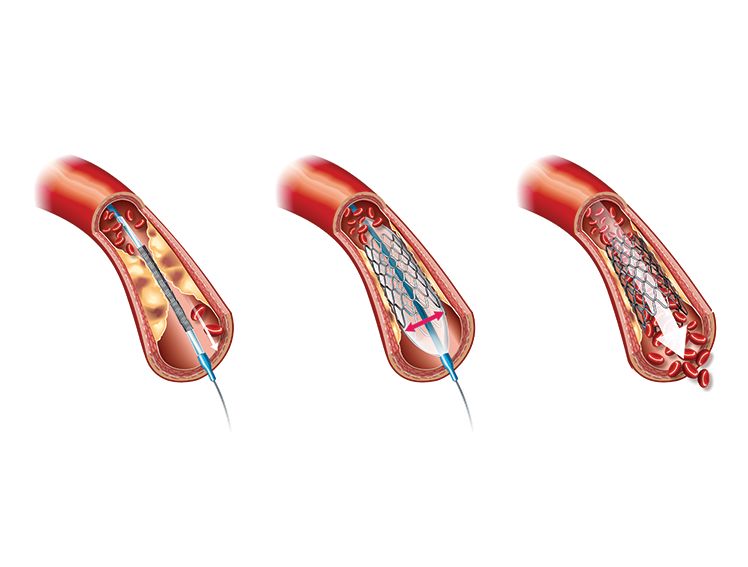
We all are aware of Angioplasty and how it can save lives and reduce heart muscle damage by restoring constant
blood flow to the heart. In recent years, Angioplasty and Stenting have shown life-enhancing and sometimes
life-saving option for a lot of people suffering from blocked arteries. It has been really effective in treating heart
attacks and strokes while improving the quality of life. And, if the success rate and worldwide acceptance of the
surgery has already convinced you to opt for Angioplasty then it is also important to know and choose the right
kind of coronary stents that adheres to ultimate efficacy and safety.
Though the modern era offers multiple designs, shapes and sizes, we've got a few tips for you that can help you
in selecting an optimal stent for a particular patient.
Evaluate efficacy
Initially, key opinion leaders (KOLs), specifically, from the West were “obsessed” with some angiographic
performance parameters associated with Drug Eluting Stents DES such as restenosis, late lumen loss, and potency of
anti-proliferative drugs present in DES in neo-intimal hyperplasia reduction within stented segments. Back then,
efficacy was “of paramount importance” to interventional cardiologists, and several evidence comparing different
DES was based primarily on their efficacy versus “more clinically relevant and vital events like repeat
revascularization.” Current experts are lucky to have numerous DES choices, fine-tuned with a majority of them
demonstrating similar effectiveness. As a result, the decision to prefer one stent over another might not be as
well-versed by comparative differences in efficacy as in the past. “With current DES, the 1-year rate of repeat
revascularization is less than 5%—almost free of the stent’s type or the type of anti-proliferative drug. It is a vivid
difference as compared to the initial scenario.” Now, the more likely relevant challenge lies in recognizing the
minute differences in outcomes among modern DES.
Considering safety
While removing the overall occurrence of blood clotting within the stent, remains an objective, modern DES
designs have reduced the event rate to such an extent, that clinicians are more confident in using DES to treat
patients previously considered at higher risk. Relative evidence now challenges the role of bare metal stents
(BMS), and this doubt is reflected across the global clinical practice. .
Thoughtful deliverability
Cardiologists opine that stent deliverability and performance are as important as safety and effectiveness when
considering multiple options. While deliverability is relevant, it is more vital to consider that though a procedure
may be more convenient with a particular device compared with another. It is not really in perspective with the
following 15 years or more for the life of the patient. So if a stent is simple to implant and works best for the
patient, it is awesome. But if the patient would gain more from a device that is a little riskier to the implant,
sharpen your skill, and face the challenge. Attention to the method will be ever more vital with approaching
acceptance of bioresorbable scaffolds in clinical practice.
Examine DAPT adherence
The debate of Bare metal stent (BMS) versus Drug Eluting Stent (DES) is not as intense as it once was, but bearing in mind the adherence factor of
blood thinner therapy after stent implantation to prevent clots and its duration might influence your decision in a
particular direction. That said, recently revised guidelines now endorse blood thinner therapy of less than 1 year in
selected patients treated with contemporary generation DES. Still, if “patients possess a high risk of bleeding or
their compliance is challenged with long-term blood thinner therapy,” BMS has traditionally been considered the
better option. However, recent evidence has challenged this belief, proposing that even with shortened DAPT
durations, modern DES have similar rates of blood clotting within the stent and superior rates of decreasing
restenosis versus BMS. “Overall, the use of BMS in clinical practice is getting reduced day by day”. Also,
observational reports indicate a lower risk of adverse events after non-cardiac surgery in patients treated with
DES versus BMS. Until more conclusive evidence can give more clear-cut answers on this issue, BMS may hold
some market share, however, their scope of use “is increasingly getting narrowed.”
Geometry matters
Geometry is the main differentiating factor among the newest-generation DES choices in terms of performance.
Their capacity for expansion? Their strut cell design? Their radial strength and scaffolding properties? If the stent
struts are thin or ultrathin, what are the chances of stent distortion? As a lot of comparative research has been
performed on stents, learning up, inside and out, on experience and knowing the geometrical structures of the
devices you use, is recommended. Thinking about stent geometry for visibility is also recommended. The thinner
the struts, the harder it is to visualize the stent”. Also, manufacturers are now ingeniously implanting metals like
iridium, molybdenum, or platinum within the devices to raise their radio-opacity.
Size appropriately
Many of the early imaging studies emphasized that, despite the angiographic look of the vessel, interventional
cardiologists frequently practice a model of geographic miss. “Here, they stent the vessel, but leave residual
disease in many segments not sufficiently covered by the stent”. So while considering stent selection, it is vital to
ascertain which device will be suitable to cover the entire diseased segment of the vessel, if possible. Allowing for
the diameter of the vessel is essential as well as the ultimate predictor of recurrent vessel narrowing with
current-generation DES, is using less than the normal size (undersized) of the stent in the vessel itself. Fitting
expansion of the stent and sizing of the stent and attaining the largest permissible minimal luminal area of the
stent are vital features in reaching the best outcomes for the patient.”
Know your polymers
DES release drugs and hence, you should be aware of each of their features and also the polymers eluting them.
Precisely knowing drug release rates, safety and efficacy profiles, and their influence on clinical outcomes are
recommended. Most current DES designs also include robust polymers that permanently stay with the stent itself.
Although new bioresorbable-polymer stents are approved for use, and other designs are in ongoing studies,
whether they will “confer an added safety or biocompatibility advantage or not, remains under study.”
Adapt for specific lesion subsets
While treating complex lesions, being aware of which stent is best for specific lesion types is recommended. “As
the playing field is currently leveled with the availability of multiple DES, it is tough to recommend a particular
stent brand for a particular lesion subset. “On the contrary, it also does not mean we should assume a
generalized approach for all DES. There are certain settings in which specific stent types have been more
extensively studied and therefore may be preferred.” So while we may not have a definitive answer on which stent
to use for each situation, attention must be paid to the full amount of data.
Develop cost sensitivity
The fact that different DES brands are now more similar than before in terms of safety and efficacy “has motivated
many different hospital programs to largely determine their inventory of stents based entirely on cost. Although
there are varied other reasons for an interventional cardiologist’s selection of one stent over another, they need to
“develop a sensitivity for costs related to the DES.” Cost depends on a hospital’s purchasing volume and also the
cost per stent. “Even with a difference of 100 per stent between two stent brands, if you are doing several
thousand procedures a year, it translates into several hundred thousand.”
Always be ready to explain your choice
It is observed that because of the design of the training programs, practitioners often learn to imitate the choices
of their teachers, especially in terms of stent selection. The presence of manufacturers’ representatives in the
catheter lab can also add confusion. But irrespective of the eventual reason for the practitioner’s choice, they
must accept the changing aspects influencing stent selection and question themselves with every case they
perform. Challenging themselves and encouraging mutual discussions as operators and colleagues “is a positive
experience that keeps them grounded in the need for science, and why they practice the way they do.” It is also
important for each interventionalist to constructively question their coworkers, even if they are more senior than
them so that everyone holds each other accountable.
It is given that as we age, the evolution in technology and science will continue to bring in more and more
effective stent choices that will have a better impact on the lives of the patients. Hence, Meril is committed to lead
innovation by developing a strong pipeline, patient centric innovative products to offer in future thus adding more
to life globally. In the end, it will be a call that will depend on a detailed study, efficacy, and safety.