
The Heart and Its Valves
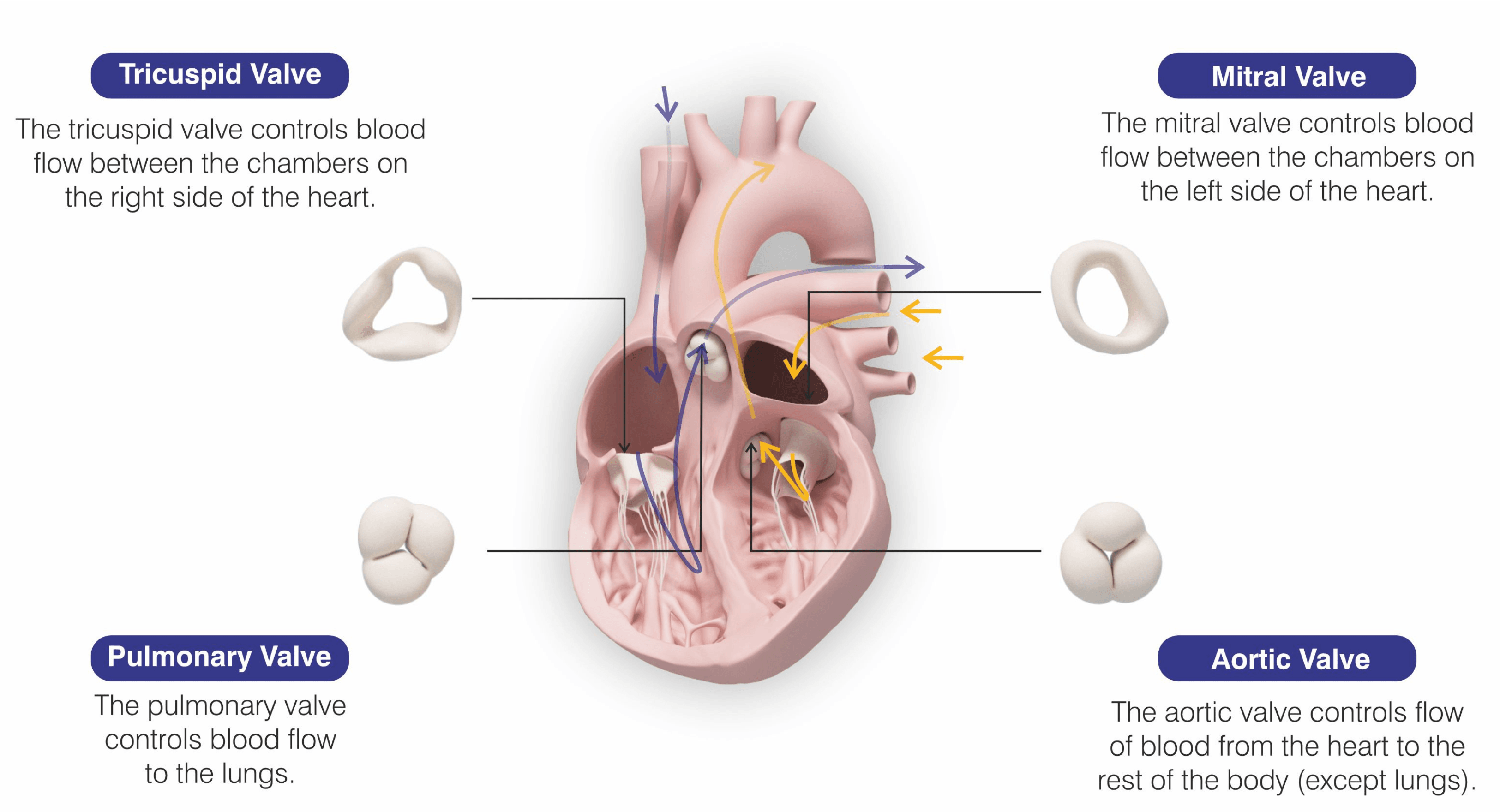
The human heart has four chambers and four valves working together to control blood flow. The valve opens to let blood flow through the heart's chambers and closes to stop blood from flowing backwards.
The mitral valve is between the left atrium and the left ventricle. It enables blood to pass from the upper to the lower chamber on the left side. It prevents any backwards flow into the atrium when the ventricle contracts.
What is Mitral Valve Regurgitation?
Mitral valve regurgitation (or mitral regurgitation (MR)) is a condition where the mitral valve does not close tightly, allowing blood to leak backward into the left atrium instead of moving forward into the aorta. This condition forces the heart to work harder to maintain proper circulation. Over time, MR can weaken the heart muscle, raise pressure in the lungs, and lead to serious complications.
Depending on the severity, MR can range from mild and manageable to severe and life-threatening. For long-term heart health, early MR detection and treatment are essential.

Symptoms of Mitral Regurgitation
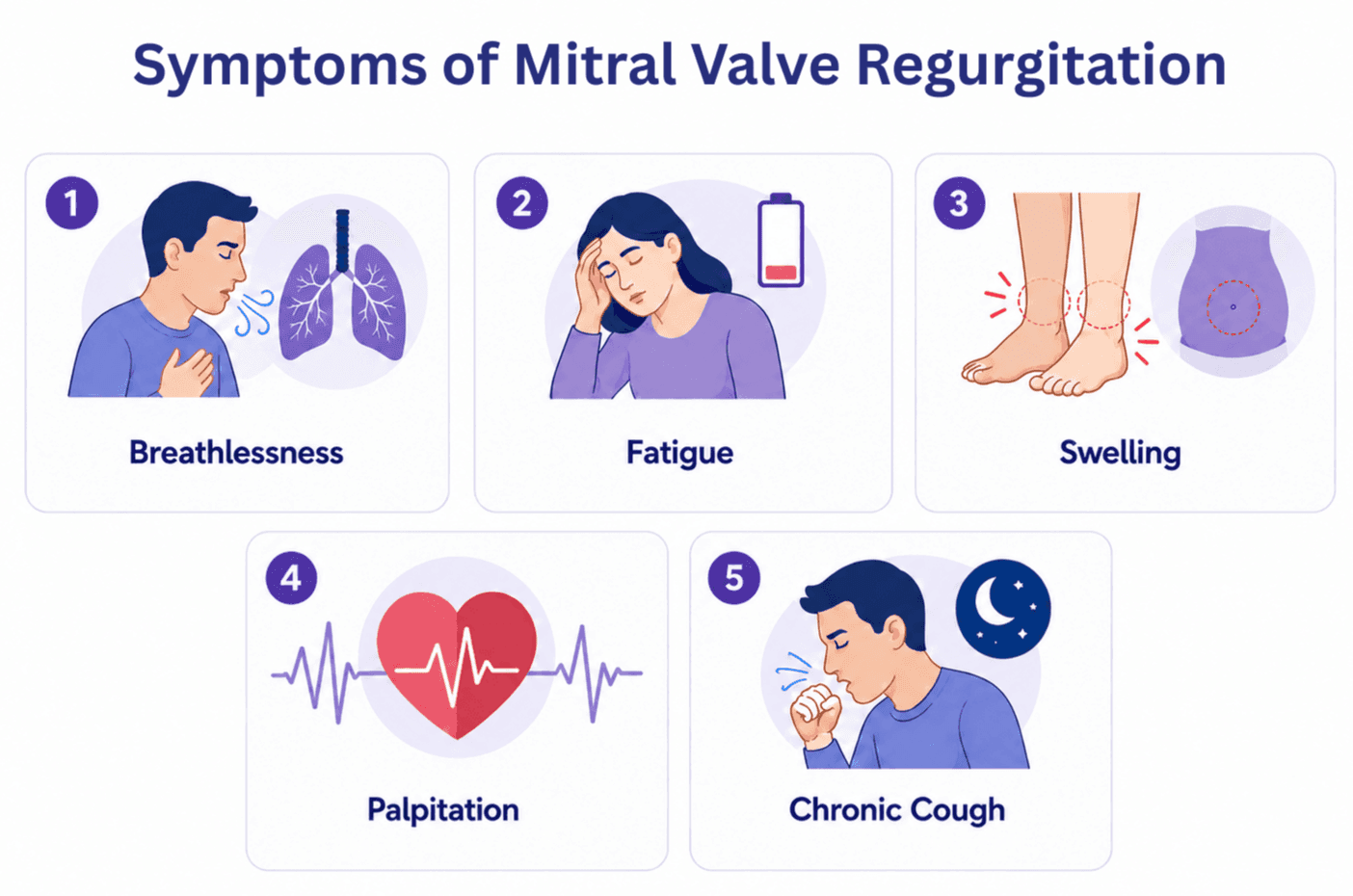
For years, people with mild MR may not experience any symptoms. Signs and symptoms of mitral regurgitation, however, could become more obvious and bothersome as the valve becomes more damaged. These include:
Breathlessness, especially when exerting oneself or when lying down
Fatigue and reduced ability to perform day to day activities
Swelling in the legs, ankles, or abdomen due to fluid buildup
Palpitations or the feeling of a fast or irregular heartbeat
Chronic cough, that usually gets worse at night or while lying down
It is essential to take these symptoms seriously and consult a doctor for a proper examination.
Causes of Mitral Regurgitation
MR can be classified based on its underlying cause:
Primary (degenerative) MR is due to direct damage or valve deterioration. Common causes include:
Age-related degeneration of valve tissue
Congenital valve defects present from birth
Infective endocarditis or rheumatic fever, which damage valve structures
Secondary (functional) MR arises when changes in the size or shape of the heart disrupt normal valve function. These may include:
Heart attacks damaging the heart muscle
Cardiomyopathy leading to heart chamber enlargement
Left ventricular dysfunction causing the valve leaflets to stretch
Complications of Untreated MR
If mitral regurgitation is left untreated, it can gradually get worse and lead to serious health issues. Some of the possible complications include:
Heart failure, as the heart struggles to pump blood effectively
Atrial fibrillation, which is an irregular and often fast heartbeat that can cause fatigue and dizziness
Pulmonary hypertension, meaning high blood pressure in the lungs, making it harder to breathe
Stroke, which may happen if blood clots form due to the heart not functioning properly
These complications can significantly impact one’s quality of life and may become life-threatening if not addressed in time.
Diagnosis of Mitral Valve Regurgitation
Doctors use physical examinations as well as diagnostic imaging to diagnose MR. The following tests are commonly used:
Stethoscope examination to detect a heart murmur
Echocardiography (TTE or TEE) to visualize valve movement and regurgitation
Electrocardiogram (ECG) to assess heart rhythm and strain
Chest X-ray to observe heart size and lung congestion
Cardiac catheterization or angiography to evaluate heart function in detail
These diagnostic tools help determine the severity of MR and guide treatment planning.
Treatment Options for Mitral Regurgitation
The severity of the illness and the patient's overall condition affect how MR is treated. Among the options are:
Medications like beta-blockers, diuretics, or vasodilators can help control symptoms
Surgical intervention to repair or replace the mitral valve is usually done through open-heart procedures.
Minimally invasive procedures like Transcatheter Edge-to-Edge Repair (TEER), which are ideal for patients who may not be fit for traditional surgery
For many high-risk or elderly patients, TEER has become a reliable and effective alternative to open-heart surgery.
When is the Right Time for TEER?
TEER is recommended in the following situations:
Patients with moderate-to-severe MR who have noticeable symptoms
Individuals whose imaging tests show strain or enlargement of heart chambers
Patients who are not suitable candidates for open-heart surgery due to age or comorbid conditions
Before irreversible heart damage occurs, early consideration of TEER significantly improves long-term outcomes.
What is TEER?
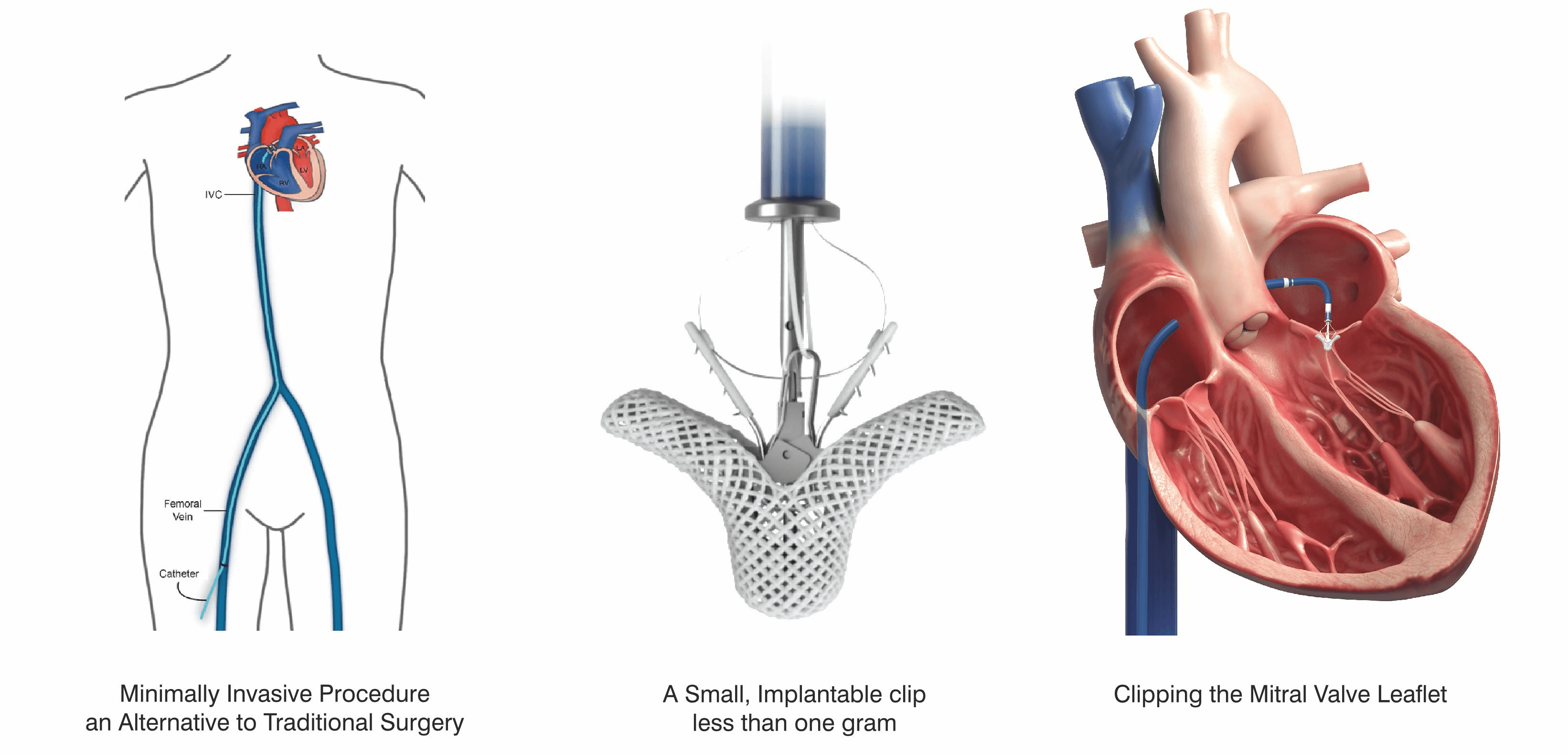
Transcatheter Edge-to-Edge Repair (TEER) is a catheter-based procedure that repairs the mitral valve without opening the chest. During this procedure, a small clip is delivered to the heart via a vein in the groin. The clip is attached to the flaps (leaflets) of the mitral valve, bringing them closer together to reduce or completely stop the backward leak.
This method is appropriate for patients who might not be able to undergo surgery because it resembles a surgical repair but is far less intrusive.
TEER Procedure: Step-by-Step
1 Pre-Procedure Preparation:
Thorough imaging with echocardiography
Routine blood tests and physical examination
Preparation in a clean, well-equipped cath lab environment with modern imaging and specialized tools.
2 During the Procedure:
The patient is sedated or under general anesthesia
A catheter is inserted through a vein in the groin and guided to the heart
Using real-time imaging, the mitral valve is accessed and the clip is positioned
Once confirmed, the clip is deployed to join the valve leaflets and reduce the leak
3 Post-Procedure Care:
One to three days of inpatient observation
Resuming everyday activities gradually
Recovery After TEER
Recovery after TEER is usually smooth and much quicker than recovery from open-heart surgery. Most patients:
Experience relief from symptoms like breathlessness and fatigue
Are discharged within a few days
Return to normal activities within 1 to 2 weeks
After the procedure, patients are advised to have routine check-ups, echocardiograms, and prescribed medications to support recovery. Lifestyle changes such as regular exercise, a low-sodium diet, and avoiding tobacco are highly recommended.
Risks and Safety of TEER
While TEER is considered safe, especially for high-risk patients, there are potential risks:
Bleeding or bruising at the catheter site
Infections
Arrhythmias or irregular heartbeat
Rare complications related to the clip placement
Despite these, TEER is supported by strong clinical evidence and has a far lower risk profile than open heart surgery.
Speak With Your Doctor
Anyone experiencing symptoms of mitral valve disease should consult a cardiologist immediately. Early detection, by routine checkups or imaging, can avoid irreversible heart damage.
All available treatment options, including TEER, should be considered by patients who have already been diagnosed with MR. Getting a second opinion or having a timely conversation with a cardiac specialist can significantly impact the results. Early intervention, informed decisions, and appropriate treatment are the most effective ways for protecting heart health and improving quality of life.
Frequently Asked Questions
How long does the TEER repair last?
Depending on the patient's condition, the repair is usually durable and lasts several years.
Is the procedure painful?
The procedure is performed under anesthesia, so the patient feels no pain during the intervention.
Who is eligible for TEER?
Patients with significant MR who are symptomatic and considered high-risk for surgery.
Is TEER better than surgery?
For many elderly or frail patients, TEER offers a safer alternative with faster recovery. However, surgical repair may still be preferred in younger, low-risk individuals.
Can TEER be performed again?
In some cases, additional clips can be placed if the regurgitation persists or returns.